


There is no right to kill your own offspring. Pregnancy is not a disease. 10.3 million British children have been assassinated by their own mothers since 1967. It’s time Eng;and stood up in front of the world and banned this grotesque barbarism so our grandchildren can remember that heroism instead.
ALEX COPPEN, OLIVER KERR, SAM THORPE
The duty of the state is to protect the good and punish the evil, not to provide a defence for evil and allow the killing of the innocent. Even if you aren’t a Christian – which is impossible if one is English because the terms are interchangeable – even Artistotle’s definition of the state as providing the “good life” can’t start by denying an innocent person the chance of one at all.
Look at any pictures of this “procedure.” Are you horrified at what you see? Found it difficult to click or go further? Wanted to turn your head away? That is because you are looking at evil.
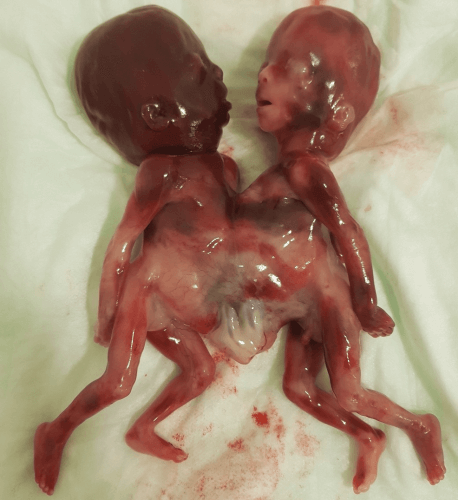
Well, you definitely wouldn’t enjoy this either. Scientists positively euphoric about killing two children deemed unlovable, worthless, and disposable: “Successful Termination of Conjoined Twins in the Second Trimester: A Case Report”.
Successful Termination of Conjoined Twins in the Second Trimester: A Case Report
You won’t want to read this either.
Many women have successfully reversed chemical abortions before taking the second pill by taking progesterone. But when Esparza told medical staff at the abortion clinic, they told her that her baby would be born with severe problems if she tried to keep it. So, she took the second pill.
“I saw my baby. No one warned me that that was even a possibility,” Esparza told reporters on Thursday. “Two weeks later, I almost died.”
In the decade before 1967, fewer than thirty people per year were convicted of procuring a miscarriage across the whole of England and Wales. Child destruction convictions—the charge applied to killing your child later—hovered near zero. The criminal law stood on the books like a Victorian monument: imposing, ancient, and almost entirely ceremonial.
Meanwhile, Parliament heard testimony of a catastrophe. Members like Roy Jenkins spoke gravely of 100,000 backstreet foeticides each year, perhaps two hundred thousand, an epidemic of coat hangers and carbolic soap in rented rooms. The disparity between enforcement and rhetoric was staggering.
A law producing thirty convictions annually was about to be reformed on the basis of statistics no one could verify, to solve a crisis no government department could measure.
Hansard records the moment MPs confronted this openly. During the Commons debate of July 1966, speakers acknowledged on the floor of the House of Commons itself:
Figures ranging from 40,000 to 200,000 have been mentioned. There is no statistical foundation for any of them.
They voted anyway.
The question is not whether Parliament acted in good faith—most members genuinely believed they were preventing harm. The question is how legislation of such magnitude passed on evidence so thin, and what happened when the law met reality.
Measurable Dead and Unmeasurable Living
What Parliament could count was mortality. The Confidential Enquiries into Maternal Deaths—the gold-standard government series—recorded approximately fifty to sixty foeticide-related deaths per year in the early 1960s. These were real women, dying from sepsis and haemorrhage (“Hospitals are devoting entire wards to the treatment of septic abortion.” HL Deb 30 November 1965), overwhelmingly poor, overwhelmingly alone. Their deaths appeared in official registers with cause codes and autopsy findings.
Against this documented tragedy stood an invisible population: the women allegedly seeking to illegally kill their offspring in their tens of thousands, whose existence was inferred rather than observed. No registry captured them. No hospital recorded those who came and went without complication. The entire edifice of reform rested on extrapolation from the visible tip of a presumed iceberg.
Parliament made a reasonable calculation. If fifty women die annually, and if death rates from amateur surgery might be one in two hundred procedures, then perhaps ten thousand illegal foeticides occur each year. If death rates are lower, perhaps twenty thousand. Push the assumptions harder—as campaigners did—and the numbers climb toward six figures.
Figures ranging from 40,000 to 200,000 have been mentioned. There is no statistical foundation for any of them.
— Hansard, HC Deb 22 July 1966
But this arithmetic worked in reverse too. If only ten thousand illegal procedures occurred annually, then legalisation would absorb them and plateau. The post-reform world would look much like the pre-reform world, merely safer.
Nobody anticipated what actually happened.
The Disastrous Effects of Decriminalisation
Official foeticide notifications for England and Wales tell the story in raw numbers:
| Year | Legal Killings |
|---|---|
| 1968 | 22,256 |
| 1969 | 54,819 |
| 1970 | 86,565 |
| 1971 | 126,777 |
| 1972 | 159,884 |
| 1973 | 167,149 |
Within five years of the Act, recorded foeticides exceeded the most generous pre-1967 estimates of illegal activity. Within a decade, they had doubled again. By 2022, England and Wales recorded over 250,000 foetus killings annually—a tenfold increase on any plausible reconstruction of pre-reform illegal incidence.
Parliament expected substitution. Women who would have sought dangerous backstreet procedures would instead receive safe medical care. The total number of killings would remain roughly constant; only the death rate would change.
What Parliament got was expansion.
Legalisation did not replace illegal foeticide with legal killing. It created an entirely new category of demand. Women who would never have risked criminal sanction, physical danger, or social disgrace now had access to a regulated, medically supervised, legally sanctioned procedure.
The economists have a term for this phenomenon: moral hazard.
When you remove the cost of an action, you change behaviour. Parliament removed medical risk, criminal liability, and much of the social stigma. Behaviour responded exactly as economic theory predicts. The surprise would have been if it hadn’t.
The Rooms Where It Happened
To understand what Parliament believed it was preventing, you must understand what backstreet foeticide actually meant. Not euphemism. Not abstraction. The physical reality.
Home Office records and medical case reports from the 1930s to the 1960s describe the methods in clinical detail.
- Uterine instrumentation with knitting needles, crochet hooks, or sharpened sticks—high perforation risk, catastrophic internal bleeding when the instrument pierced the uterine wall into the abdominal cavity.
- Intrauterine instillation of soap solutions, caustic enough to destroy tissue on contact, inducing chemical necrosis, renal failure, toxic shock.
- Potassium permanganate tablets inserted directly into the cervix, burning through tissue, creating wounds prone to fatal infection.
- Syringes filled with carbolic acid.
- Slippery elm bark forced into the cervical canal.
- Quinine in doses approaching toxicity.
The septic maternal wards of major hospitals told the aftermath. Women arriving in extremis with raging fevers, abdominal rigidity, spreading peritonitis. Emergency hysterectomies performed on patients who would never bear children again. Blood transfusions measured in pints. Long inpatient stays for those who survived. And for those who did not, death certificates recording septicaemia, haemorrhage, air embolism, perforated uterus.
The House of Lords debate of November 1965 includes the memorable line about not substituting “the scalpel for the knitting needle.” The imagery was not rhetorical flourish. It was descriptive accuracy.
Parliament saw these horrors and concluded—reasonably—they must be stopped. The error was not in the diagnosis of suffering. The error was in assuming legalisation would merely relocate existing procedures rather than multiply them beyond recognition.
The Backstreet Abortionist: A Profile
To understand the reformers’ mental model, consider who they believed they were legislating against.
Home Office records paint a remarkably consistent portrait of the prosecuted “abortionist.” She—almost always she—was typically a woman aged forty to sixty-five, often widowed or unmarried, usually working-class, frequently a former midwife or maternity aide. She operated from her own home or a rented room, charged cash fees, and was known locally by reputation built over years of repeat custom.
Police files note repeatedly:
Many of those convicted had previous convictions for the same offence.
This was not casual criminality but semi-professional commerce, reputation-based, and geographically concentrated in major cities. Officers often only intervened after death or serious injury prompted hospital referral.
Parliament looked at this pattern and saw predatory exploitation. Elderly women profiting from desperation, offering dangerous services to the vulnerable, escaping justice until someone died. The debate framing cast legal killing a child as rescue: removing criminal exploitation by absorbing demand into the medical system.
What this framing missed was elementary market logic. The backstreet “abortionist” existed because demand existed. She did not create demand; she served it, badly. Eliminating her did not eliminate the underlying pressure—it merely redirected it. And once the redirect occurred, it became clear the pressure was far larger than anyone had measured.
The Strange Clause Nobody Discusses
Liberal MP David Steel introduced the Medical Termination of Pregnancy Bill as a Private Member’s Bill after winning a ballot slot in 1966. Yes, the same mechanism gamed exploited by Romanian migrant Sydney Silverman of the Labour party to vandalise British customs he did not share in his own lineage. Steel himself was relatively young and not a cabinet minister, but used the private members’ process to get the issue onto the Commons agenda.
It is one of the shortest and most atrocious pieces of legislation ever passed by Parliament, and virtually no-one has ever read it.
Deep in Section 1 of the Abortion Act lies a phrase so anomalous it deserves examination: killing of a child is permitted where continuation of pregnancy would involve risk to:
the physical or mental health of the pregnant woman or any existing children of her family.
Existing children. Not the woman herself. Her other offspring.
This is not medical language. A physician assessing patient health does not normally factor in the welfare of siblings. This is social-work language, imported wholesale from pre-1967 psychiatric practice where doctors had justified the killing of one’s offspring by reference to “family stability” and “inability to cope.”
Parliament codified existing clinical custom without noticing it had fundamentally altered the law’s character. What began as emergency medical exception—preserving maternal life—became discretionary welfare judgement.
A doctor could now certify foeticide on the grounds it might benefit children who already existed, invoking predicted social consequences rather than present medical necessity.
By the early 1970s, over ninety per cent of foetus killings relied on the mental health provisions. The clause designed for psychiatric emergencies had become the standard pathway for routine procedures. The Act’s architecture made prosecution virtually impossible: once two doctors signed the statutory form, no court could second-guess clinical judgement about predicted mental health outcomes.
Parliament built a defence so broad it swallowed the offence entirely.
Procuring Miscarriage Remains Illegal In England
Here is a fact often forgotten: paying a doctor to kill your child remains a criminal offence in England and Wales. The Offences Against the Person Act 1861 was never repealed. Section 58 still criminalises procuring a miscarriage. The maximum penalty remains life imprisonment.
What the 1967 Act created was not legalisation but exemption. Doctors who comply with statutory requirements receive immunity from prosecution. The underlying prohibition stands untouched, a legal fossil preserved in amber while practice evolved around it.
This peculiar structure was deliberate. Parliament in 1967 wanted maximum change in medical practice with minimum change to moral and criminal law. Members could vote for reform while telling constituents they had not “legalised abortion”—technically true, if practically meaningless.
The architecture reveals the political bargain. Opponents were mollified by formal retention of illegality. Supporters obtained functional access through medical gatekeeping. Neither side confronted the fundamental question: is the unborn child a human being with moral status? The law’s elaborate procedural machinery exists precisely to avoid answering.
The First Technocratic Intervention
Step back from “abortion” specifically and a larger pattern emerges. Until the mid-twentieth century, Western medicine had a stable purpose: treating pathology. Physicians cured disease, repaired injury, restored normal function. Even major interventions—surgery, antibiotics, transfusion—aimed at returning the body to its natural baseline. Something has gone wrong; let us fix it.
The post-1960 shift represented something genuinely new. Nothing is wrong; let us change it anyway.
Hormonal contraception, elective foeticide, sterilisation on demand, later IVF and hormone replacement—these were not corrections of disease. They were interventions in healthy biological processes, undertaken to produce preferred social outcomes.
Pregnancy is not a disease. It is not an injury or infection or malfunction. It is the normal operation of human reproductive biology. When medicine intervenes to terminate pregnancy, it is not treating pathology but overriding function. The physician becomes not healer but technician, applying expertise to produce a specified result regardless of biological trajectory.
Legal foeticide was the first large-scale instance of this transformation. Not the last—”gender medicine,” “enhancement” pharmacology, life “extension” research all followed the same logic—but the first. Once medicine accepted authority to override healthy function in pursuit of social preference, the conceptual barrier fell. Everything else became negotiation over boundaries.
The Abortion Act did not merely change law. It authorised a new relationship between human beings and their bodies, one mediated by expertise and procedure rather than nature and obligation. This was the moment biology ceased to be fate and became a policy problem.
Technocracy Masks Evil as Process
Once something becomes a form, responsibility fragments. Guilt dissolves. Agency disappears.
- No one kills. The system “permits.”
- No one chooses. The committee “authorises.”
- No one bears moral weight. The procedure “meets criteria.”
Consider the shift in language the new regime required:
- Killing became “termination”—an ending, unspecified.
- Child became “product of conception”—biological material, categorically distinct from baby.
- Death became “healthcare”—placing the act alongside vaccination and dental checkups.
- Conscience became “access”—framing destruction as freedom, opposition as oppression.
- Moral dilemma became “clinical indication”—a box on a form.
This is not accidental euphemism. It is how bureaucratic systems neutralise moral resistance. When a society cannot name what it does, it cannot think clearly about whether to continue. The vocabulary of moral clarity has been defined out of legitimate conversation.
Hannah Arendt identified the same mechanism in entirely different circumstances: evil becomes ordinary not because people become monsters, but because responsibility dissolves into process. No one intends catastrophe. Everyone follows procedure. The outcome emerges from the system rather than from wills.
The horror is not dramatic. It is administrative. That is what makes it so difficult to see, and so impossible to stop.
Soviet Descent Into Population Hell
Britain was not the first country to travel this road. The Soviet Union legalised foeticide in November 1920, becoming the first nation in history to do so.
Lenin’s decree framed the measure as temporary necessity.
As long as the moral survivals of the past and difficult economic conditions persist, women will inevitably resort to abortion.
The assumption was explicit: once socialism produced material abundance, women would choose motherhood freely and child killing would fade away.
By 1926, official Soviet data recorded 885 foeticides per thousand live births in major cities—nearly one killing for every birth. The promised withering never came. Stalin, alarmed by demographic collapse and labour shortages, re-criminalised foeticide in 1936, explicitly citing “the strength of the socialist state” as justification.
After Stalin’s death, Khrushchev legalised foetcide again in 1955. What followed was the most comprehensive demographic study in its effects available anywhere. Soviet health ministry statistics from the 1960s to the 1980s show:
| Year | Killings | Live Births |
|---|---|---|
| 1965 | ~5.6 million | ~4.6 million |
| 1980 | ~7.0 million | ~5.0 million |
| 1987 | ~8.1 million | ~5.6 million |
For much of the late Soviet period, killing outnumbered births. The average Soviet woman killed between five and ten of her children in her lifetime. Modern contraception was scarce; foeticide became, in the demographers’ clinical phrase, “a substitute for contraception.”
The Soviet rate exceeded Western Europe’s by five to ten times. By the USSR’s collapse in 1991, total fertility had fallen below replacement and population momentum had turned negative. Russia’s population declined by six million in the 1990s alone.
Different ideology, different economic system, different political structure—same outcome. The mechanism was not Marxism. It was the removal of friction from a behaviour sensitive to incentives.
The Marxist Logic Behind “Family Planning”
Why did communist ideology produce child killing legalisation before any liberal democracy? The answer lies in Marxist theory about family, labour, and the state.
Orthodox Marxism viewed the bourgeois family as an economic institution: a mechanism for transmitting private property, reproducing labour power, socialising obedience, perpetuating inheritance. Engels called the modern family:
founded on the open or concealed domestic slavery of the wife.
Family structure was not moral unit but economic technology.
Leninist economics required maximum female participation in production. Women were defined primarily as labour units. Pregnancy meant temporary withdrawal from the workforce—structural inefficiency in a system demanding total mobilisation. “So long as woman is burdened with housework,” Lenin wrote, “her position remains a slave’s.”
Children were considered a collective responsibility. Early Bolshevik ideology held children should be raised by the state, emotional dependence on family was pre-socialist, loyalty should transfer from parents to Party.
From within this logic, killing followed inevitably. If motherhood is not sacred, if the family is not foundational, if labour supply must be flexible, if women must not be bound to reproduction—then forcing childbirth becomes reactionary.
The USSR did not promote foeticide ideologically. It simply became the default fertility-control mechanism of the planned family in a planned economy hostile to the structures within which reproduction makes sense. The system did not hate children. It merely stopped caring about them.
The demographic damage persisted into the post-Soviet era and continues today. A civilisation cannot recover fertility once the institutions supporting it have been dismantled. The Soviet experiment proved this at continental scale.
Moral Hazard at Population Scale
Parliament in 1967 believed it was addressing a medical safety problem. Soviet planners in 1920 believed they were managing labour-force efficiency. Neither anticipated sustained, multi-decade, population-level behavioural change.
The error was identical in both cases. Legislators treated foeticide as a discrete intervention with bounded effects. They did not recognise it as a parameter in a dynamic system where behaviour responds continuously to incentives.
Lower medical risk means more procedures. Lower legal risk means more procedures. Lower social stigma means more procedures. Each reduction in cost produces additional demand. The system does not equilibrate at “replacement”—illegal killings replaced by legal ones—but continues expanding until other constraints bind.
What constraints? In the Soviet case, virtually none: foeticide was free, fast, and state-provided. In Britain, the constraints were softer—two-doctor certification, hospital allocation, social residue of disapproval—but progressively weakened over decades. Waiting times shortened. Private clinics emerged. Telemedicine arrived. Each reduction in friction produced the predictable response.
In Britain, the moral hazard operated at the personal level: individual women responding rationally to changed incentives, individual decisions aggregating into population-level effects neither intended nor foreseen.
In the Soviet Union, the moral hazard operated at the institutional level: the state itself behaved irresponsibly, prioritising short-term labour efficiency while externalising long-term demographic consequences to future generations who had no voice in the decision.
Same mechanism. Different point of application. Both catastrophic.
Every Argument For This Evil Fails
Strip away the procedural complexity, the medical terminology, the rights language, and every debate about foeticide reduces to a single question: is the unborn child a human being with moral status?
If no, then foeticide requires no justification. Remove what has no value and nothing is lost.
If yes, then no justification is sufficient. Hardship does not authorise killing. Convenience does not authorise killing. Even genuine tragedy does not authorise killing.
Every secondary argument—viability, consciousness, pain perception, dependency, economic circumstance—functions to avoid this binary. Each offers a criterion for moral status conveniently excluding the unborn while purporting to rest on principle.
But the criteria never hold.
- “It’s not a life.” It’s alive, human, and growing—biology defines life as a living human organism, and embryos meet every criterion. What you mean is you don’t think it counts yet.
- “It’s just a clump of cells.” So are you. All humans are clumps of cells. Uniqueness comes from organisation, not size or appearance.
- “Life begins at birth.” Nothing magical happens at the birth canal except a change of scenery. Birth changes location, not biology.
- “Life begins at consciousness.” Consciousness is intermittent. Sleeping, anaesthetised, or comatose humans would lose moral status. We do not kill them either.
- “It can’t survive independently.” No human is independent. Infants require total care. Dependency does not erase humanity.
- “It can’t feel pain.” Pain sensitivity is not a prerequisite for moral status. Painless killing is still killing.
- “It can’t reproduce.” By this definition, children, infertile adults, and post-menopausal women are non-life. The criterion is absurd.
- “It’s not a person.” If personhood is granted by law or opinion, then rights become conditional and revocable. Every atrocity in history began by deciding some humans weren’t persons.
The arguments mutate because they must. Each, when pressed, collapses into ad hoc special pleading. What remains is the unstated premise: some human beings may be killed because their existence is inconvenient to others.
Stated plainly, the premise is monstrous. So it is never stated plainly.

••••
The Liberty Beacon Project is now expanding at a near exponential rate, and for this we are grateful and excited! But we must also be practical. For 7 years we have not asked for any donations, and have built this project with our own funds as we grew. We are now experiencing ever increasing growing pains due to the large number of websites and projects we represent. So we have just installed donation buttons on our websites and ask that you consider this when you visit them. Nothing is too small. We thank you for all your support and your considerations … (TLB)
••••
Comment Policy: As a privately owned web site, we reserve the right to remove comments that contain spam, advertising, vulgarity, threats of violence, racism, or personal/abusive attacks on other users. This also applies to trolling, the use of more than one alias, or just intentional mischief. Enforcement of this policy is at the discretion of this websites administrators. Repeat offenders may be blocked or permanently banned without prior warning.
••••
Disclaimer: TLB websites contain copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available to our readers under the provisions of “fair use” in an effort to advance a better understanding of political, health, economic and social issues. The material on this site is distributed without profit to those who have expressed a prior interest in receiving it for research and educational purposes. If you wish to use copyrighted material for purposes other than “fair use” you must request permission from the copyright owner.
••••
Disclaimer: The information and opinions shared are for informational purposes only including, but not limited to, text, graphics, images and other material are not intended as medical advice or instruction. Nothing mentioned is intended to be a substitute for professional medical advice, diagnosis or treatment.
Disclaimer: The views and opinions expressed in this article are those of the author and do not necessarily reflect the official policy or position of The Liberty Beacon Project.



